
Say the word “coroner” and people think of homicides and other violent deaths. The truth? A significant but variable proportion—about 24 to 50 percent—of accepted or jurisdictional deaths in medicolegal death investigation offices are natural in manner.
Many natural deaths are due to diabetes or diabetes-associated diseases like heart disease or kidney failure. Type 1 diabetes accounts for 5-10 percent of adult diabetes cases in the U.S. By extrapolation, Type 2 diabetes accounts for 90-95 percent of diagnosed adult diabetes cases. But coroners also need to be aware of a third type of diabetes.
Latent autoimmune diabetes of adulthood (LADA)
Type 1.5 or latent autoimmune diabetes of adulthood (LADA) seems to be on the rise. In its early stages, health care providers often diagnose and treat LADA as Type 2 diabetes. But, like Type 1 diabetes, LADA has an autoimmune component. Most experts believe an autoimmune reaction is responsible for the gradual loss of pancreatic beta cell function in LADA. Eventually, the beta cells produce insufficient insulin to sustain life, and the patient requires exogenous insulin.
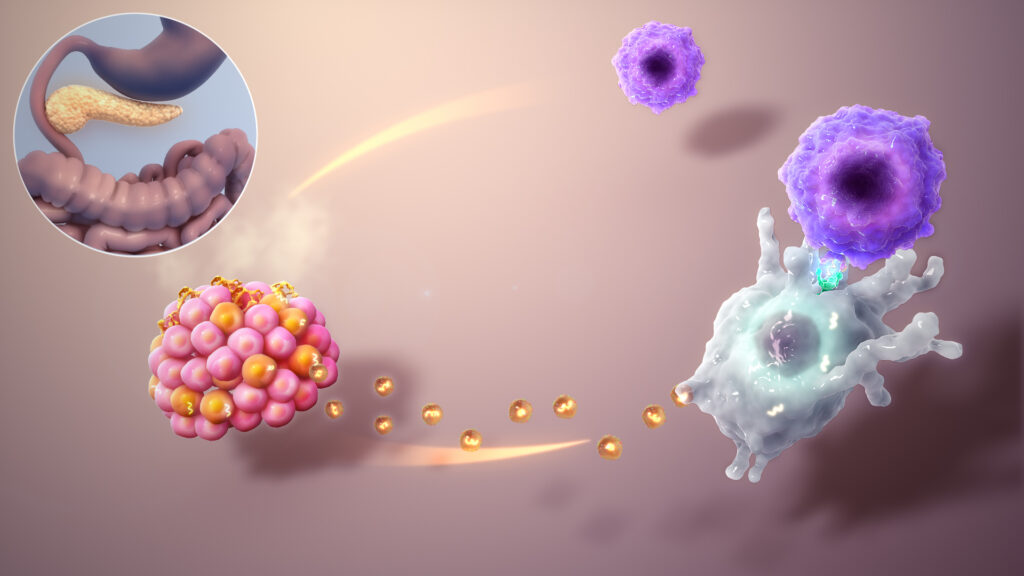
The graphic illustrates an autoimmune-type attack in which proteins (yellow dots) secreted by the beta cells (orange cluster) are mistakenly taken up by dendritic cells (big whitish cell). When the dendritic cells present the proteins to the T-cells (smaller purple-blue cells), the T-Cells treat those proteins as enemies and attack their source, the beta cells. (The upper abdominal location of the pancreas is shown within the circle.)
The clinical picture, along with serological tests confirming the presence of certain autoantibodies, especially GAD-65, can help predict whether Type 2 diabetes will progress to LADA. But sometimes health care providers miss the signs of progression, continue to treat such patients for Type 2 diabetes, and do not prescribe insulin. Without insulin, patients with LADA can develop diabetic ketoacidosis (DKA), a medical emergency. DKA is characterized by very high glucose levels, ketosis, and acidosis. When recognized, it is treatable and has a low in-hospital mortality rate.
But when the gradual transition from Type 2 to Type 1 diabetes in a LADA patient isn’t recognized or treated correctly, DKA can be fatal. Sometimes, as in the two cases described below, it’s the coroner who makes the diagnosis.
Case 1: Misdiagnosis of LADA
In July of 2020, S. D.’s employer requested a well-being check. Police found the mid-fifties man dead in his home, but did not find the circumstances suspicious.
The deputy coroner observed the body of a thin man — estimated weight 130 pounds — with resolving rigor mortis. According to his family, S.D. had a history of diabetes and was struggling with unintentional weight loss The weight loss had cost him his manual labor job and thus his health insurance.
At his last doctor’s visit approximately half a year earlier, S.D.’s hemoglobin A1C was 14.9, a “major concern.” The practice had treated him for Type 2 diabetes for many years, most recently with two oral medications, metformin and glipizide. S.D. had lost 30 pounds over the past year. Neither the A1c nor the weight loss prompted a change in treatment.
A PCR swab test for COVID was negative. The vitreous glucose, from a specimen drawn 24-36 hours after death, was 368 mg/dL. Normal, according to the lab, was < 200 mg/dL, but even a total absence of glucose in postmortem vitreous is not unusual. The femoral blood beta hydroxybutyric acid level was 1000 mcg/mL (normal less than 50), and the acetone level was 40 mg/dL (normal, up to 3).
Cause of death: Diabetic ketoacidosis due to Type 1 diabetes mellitus due to latent autoimmune diabetes in adulthood (LADA).
Case 2: LADA mistreated as Type 2 diabetes
In early 2021, a family member found M.W., a sixty-something man, dead at home. Seven years earlier, M.W., then in his late-fifties, had a blood glucose of 673 mg/dL (normal 65-99) and a hemoglobin A1c of 17.7% (normal less than 5.7%). The doctor’s note said that M.W. had “diabetes 1.5, managed as type 2.” His only diabetes medication was oral metformin, usually prescribed for prevention or treatment of type 2 diabetes.
A physician who had seen M.W. for back pain five years ago understandably refused to sign the death certificate. An electronic records search failed to identify a more recent medical provider or more recent laboratory tests.
The coroner accepted the case, testing for COVID (negative) and drawing toxicology samples to confirm a suspected postmortem diagnosis of diabetic ketoacidosis. The vitreous glucose, drawn approximately 24 hours after death, was 480 mg/dL. The femoral blood beta hydroxybutyrate level was 960 mcg/mL, and the acetone level was 44 mg/dL.
Cause of death: Diabetic ketoacidosis due to latent autoimmune diabetes in adulthood (LADA)
The coroner’s role in postmortem diagnosis of diabetic ketoacidosis and LADA
The coroner did not need to perform an autopsy in either of these cases. The case history, external examination, and physical and laboratory testing sufficed to determine diabetic ketoacidosis as the cause of death.
Vitreous electrolyte and glucose testing is essential to the postmortem diagnosis of diabetes. Femoral blood testing for beta hydroxybutyrate and acetone is essential for diagnosis of ketosis. If both are elevated, the coroner can make a postmortem diagnosis of diabetic ketoacidosis with a high degree of medical certainty.
Postmortem autoantibody testing for GAD-65 is not an established practice and not necessary in most cases. In the deaths described above, clinical and recent medical history were consistent with LADA or Type 1 diabetes misdiagnosed and/or mistreated as Type 2.
The lives of both S.D. and M.W. could have been saved if someone had been available to call an ambulance, but they lived alone and died during the COVID-19 pandemic. Their lives might also have been saved if their health care providers had correctly diagnosed and treated their LADA/Type 1 diabetes. The most difficult task for the coroner may be explaining the cause of such preventable deaths to the next of kin.
Pandemic effect on deaths due to diabetic ketoacidosis
National (U.S.) data show that DKA‐related deaths surged in 2020 and rose again in 2021. Possible reasons include changes in health-care access, reluctance to seek health care, loss of insurance, stress, isolation, COVID infections precipitating DKA, and diversion of health care resources to the COVID emergency.
This suggests that coroners may be responsible for an increased number of natural death certifications during future public health emergencies, including natural disasters. As happened during the COVID-19 pandemic, medicolegal death investigation offices may have to limit autopsies to criminal or other suspicious deaths. Therefore, coroners without medical training should know when to suspect diabetes and how to make a postmortem diagnosis of diabetic ketoacidosis using history, physical findings, and specific toxicological tests.
I’ll be writing more about diabetes, insulin, and medicolegal death investigation in future posts. To be notified by email, sign up for my monthly newsletter (link in sidebar).
Featured image credit: Mangocove, CC BY-SA 4.0 via Wikimedia Commons
The information provided on this website is for educational purposes only and is not intended as medical advice. Always consult a qualified healthcare provider before making any health decisions.